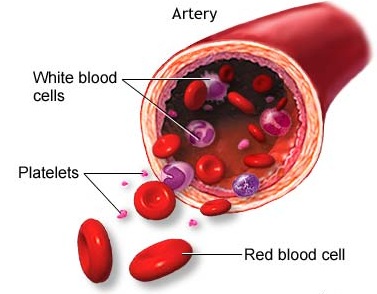
So far we’ve talked about our blood, it’s parts and functions, leukemia, lymphoma and myeloma. Today we will start covering Myeloproliferative Neoplasms. (No, you’re not having deja vu…the post below is a re-post from earlier in my blog)
I have been asked what exactly an MPN is by many people: friends, family, co-workers random strangers at the doctor’s office(so, what are YOU in for…?)… and I have struggled over the years with finding a good way to explain it. I have come up with a couple of silly analogies about a factory going haywire and I also dabble with the more technical explanations from time to time…but that tends to leave me with blank stares… or they smile and nod along with me, meanwhile I can see the information going in one ear and out the other……
In this first of four articles, I am going to try to find concise ways to explain MPNs as a whole. In the subsequent entries I will try to do the same for each ET, PV and MF.
SO…here goes.
If we break down the words they give a pretty good working definition.
Myeloproliferative Neoplasm:
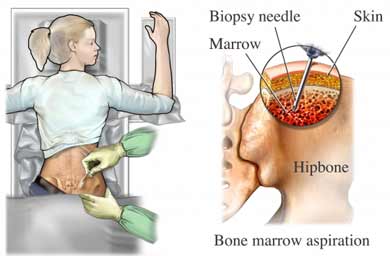
Myelo -From the Greek Muelos which means marrow
Proliferative/Proliferation -to grow or multiply by rapidly producing new tissue
Neoplasm – an abnormal growth of body tissue
So basically…the bone marrow produces lots and lots of cells that do not belong there. That is my basic working definition of a Myeloproliferative Neoplasm. It’s simple, not very technical, and it doesn’t tend to leave people’s eyes glazed over. For a lot of people, that is a fine answer, and they don’t need to know anything else.
Others want to know more, though. How did you find out about/were diagnosed with that disease/condition/thing, “is it …you know….(whisper)cancer?”, how do they treat it, when will it be cured, etc etc….Come to think of it…those are all questions that patients ask too. I have probably asked all of these questions a few times. I’ll try and answer these the way they were explained to me, and the way I understand them…so…these words might not make any sense whatsoever once they exit my head….
We’ll start with the first question. How is one diagnosed? From what I have seen, read, and heard from other patients, an MPN diagnosis is typically secondary to another condition/event. I do not know statistics on this at the moment, but the majority of people I have spoken to were diagnosed after a heart attack, stroke or blood clot. That is not the only way these diseases are diagnosed. Sometimes they are discovered during routine blood work, or during a physical, but more commonly they are diagnosed after a major event. Part of the reason for this could be that symptoms of MPNs are fairly generic, and that makes it difficult to pinpoint their origin. For example I had bruising, headaches and fatigue. Put those three symptoms into a web search…and you’ll come up with 4,310,000 search results. If you pull up one of those Internet Diagnostic Websites(I won’t use the name here…but I bet you all know what I mean…) it pulls up 127 different possible diagnoses, from acute stress to cat scratch fever… So it’s easy to see why someone could go undiagnosed for a while. Once it is narrowed down to an MPN, there are different diagnostic criteria for each of the different conditions. The doctor will use these criteria to determine diagnosis and from there he or she will decide on the patient’s treatment.
“Is it…you know…(whisper) cancer?” I have never understood why people get so reverent, (or I guess fearful is more likely) of a word? Is it going to jump out and infect you if it hears you speak of it? Don’t worry, it can’t hear you…you can say the word. This is a bit of a touchy subject though. By its most basic definition (a disease caused by an uncontrolled division of abnormal cells), then sure. MPNs are a kind of cancer. They are not generally defined as malignant (the tendency of a condition to be come progressively worse, and eventually lead to death) conditions though. (unless they are positive for the Philadelphia Chromosome, in which case you are most likely looking at Chronic myelogenous leukemia– which is another issue unto itself) Prior to the 2008 decision by the World Health Organizations, we called these conditions MPDs Myeloproliferative DISORDERS. There are people who feel that after the WHO changed the classification from Myeloproliferative DISORDERS to Myeloproliferative NEOPLASMS, that somehow they have magically become something else. That isn’t true. The fundamental nature of the diseases has not changed. What has changed is their classification. (Which almost seems to have been done for coding/paperwork purposes really) MPNs contain many of the same symptoms that you might see in a lot of different diseases, so instead of leaving them off in their own lonely little category, they have been lumped in with everything else. For some people the word “cancer” is very intimidating, so they prefer not to have it attached to their condition, which is fine. To me though, cancer is just a word. It won’t jump out and bite you, nor should you allow it to affect your outlook on your treatment.
As far as treatment goes, this will vary by disease, and also by patient. Treatments can include anything from watch and wait and periodic blood work all the way up to a bone marrow transplant. I will get more in depth about treatments in the next few articles. In some cases the treatment is almost worse than the symptoms of the disease that it treats (which is true for pretty much any disease). There are some people who feel that holistic treatments are the way to go. Honestly, I don’t know much about holistic treatments, and (as narrow minded as this may be…) I personally feel more comfortable sticking with conventional scientific methods. I know I know… “why do you want to put those nasty chemicals in your body…?” Well, those nasty chemicals have been through many years of clinical trials, countless tests, reviewed by hundreds of patients, doctors, clinicians, and scientists, and that’s just how I feel comfortable. It may be different for others, and I encourage them to seek out the (well researched, please) therapy that they are comfortable with.
When will I be cured? Well, that’s a good question with a simple answer. I won’t be cured. MPNs are chronic diseases. The way my doc puts it “Plan to live a long life with this”. Well that’s comforting…sort of. All the doctors I have seen (1 hem/onc who had never seen an MPN before in his practice, and 2 very well respected hem/oncs who deal almost entirely with MPN patients) all tell me that yes, I will have ET forever, but that it will almost certainly NOT be the cause of my ultimate demise. The majority of MPN patients that I know who have passed away over the years did NOT die of anything to do with their MPN diagnosis. Most died of old age, some were complications of another disease,, etc. That is not to say that MPNs can not cause death, or that they are not serious. They are. Owing to the difficulty in diagnosis, MPNs have probably caused more deaths than we know about. Even though these diseases are not “curable” exactly, you can still live a nice full happy life, with minimal intrusion from your disease once you have gotten the proper treatment.
So there it is. That is my very general outline, and answers to the basic questions that I have heard most often. Over the next few weeks I will be getting more specific about the types of MPNs ET, PV, and MF. Stay tuned for the next entries!
Tomorrow we will talk about Polycythemia Vera (PV)
Until tomorrow,
Lina